Recently, the Centers for Disease Control and Prevention (CDC) revised its COVID-19 recommendations to eliminate the quarantine for infected people. Previously this had been reduced from 10 to 5 days. It is now not recommended at all, although masking for 5-10 days is still recommended after being infected, and there are suggestions -- “strategies that people may want to consider in order to reduce their risk” – such as avoiding crowded areas and maintaining a distance from others.
‘“We know that Covid-19 is here to stay,” Greta Massetti, a C.D.C. epidemiologist, said at a news briefing on Thursday,’ which about sums up their perspective. It is apparently their justification for the (lack of) safety recommendations and precautions. The author of the article notes that the loosening of the guidelines free ‘schools and businesses from the onus of requiring unvaccinated people exposed to the virus to quarantine at home.’
As far as that author (Emily Anthes) and the editors are concerned, there seems to be universal approval of this change from the medical and epidemiologic community, at least based upon those that are quoted in the article:
‘“I think they are attempting to meet up with the reality that everyone in the public is pretty much done with this pandemic,” said Michael T. Osterholm, an infectious disease expert at the University of Minnesota’;
‘“I think this a welcome change,” said Amesh Adalja, a senior scholar at the Johns Hopkins Center for Health Security. “It actually shows how far we’ve come”’ ;
‘“This really will help to minimize the impact of Covid-19 on education,” said Christina Ramirez, a biostatistician at the University of California, Los Angeles.’
One commentator, ‘Mercedes Carnethon, an epidemiologist at the Northwestern University Feinberg School of Medicine, said that she did not view the changes, even the elimination of quarantines in favor of 10 days of masking, as a loosening of the agency’s guidance.’
Dr. Carnethon continues ‘“We certainly know that wearing a high-quality mask is going to provide some of the strongest protection against spreading it to somebody else, and quarantine is logistically burdensome. That could be seen as a relaxing of guidelines, but I think it’s a much more appropriate and targeted solution.” Except, of course, that the CDC is not recommending that we mask in public areas. Whoops.
Ross Douthat, NY Times Op-Ed columnist, writes (Aug 13, 2022) that “The CDC continues to lead from behind”. His take is essentially that “everyone” has already been doing (or not doing) the things that the CDC is now recommending (or not recommending). I would agree that that is true (at least in the US), but to me it suggests that the recommendations are driven politically, not by “the science”. Certainly it has been “an onus” for schools and businesses to comply with the recommendations (often conflicting) from different governmental agencies and others to protect their students, staffs, and customers. People do not like having to wear a mask in public, even in crowded indoor spaces, nor having to distance, nor staying home and quarantining and missing school or work. Or, even missing social interactions, from casual to parties. If CDC is “leading from behind”, making recommendations that much of the population has already been implementing, then this new step will encourage those who have already been doing so to further relax their carefulness. They may do so from a desire to get an education, make a living, interact with family and friends, or to party and use drugs or have wild sex, but these are, essentially, quantitative and not qualitative, differences. The fact that the article in the Times could not (or at least did not) find any countervailing views from epidemiologists, scientists, physicians, and other experts further endorses the “opening up” that people want. It is political in that having restrictive requirements is generally unpopular and could lose votes for politicians.
The only problem, of course, is that COVID is still out there and we are still at risk. What we are at risk for varies a lot, depending upon who we are, from “mild” illness (usually not so mild!) to severe illness to hospitalization, to death. The people who are most at risk are those who are immune compromised, either because of age, or illness, or (my favorite) the drugs that they are taking to treat illness, including the drugs widely advertised on television for cancer and rheumatic diseases. Plus anyone, of any age or prior health status, can get “long COVID”, with persisting symptoms that can be very severe and debilitating.
The World Health Organization observes that “7.9 billion people” (the world’s population) are still at risk for COVID, and that thousands are still dying every week. This poster makes those points, and also that new variants continue to emerge and can quickly become dominant. It also recommends things like keeping your distance and wearing a mask, abandoned by most Americans.

Of course, the risk of COVID also varies from country to country, which could justify why WHO and CDC have different recommendations. After all, in some countries there is greater risk than in others, and the struggle is just to keep their people alive. This might be reassuring to Americans if it were not for the fact that the US is one of those, remaining the leader in deaths.
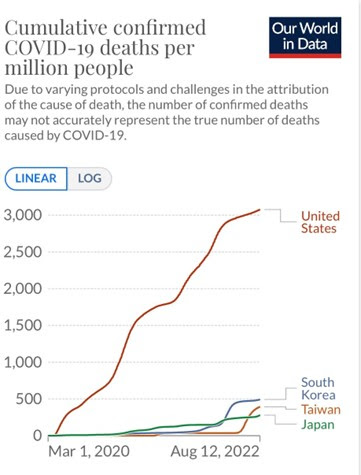
(https://ourworldindata.org/coronavirus)
One of the key determinants of how a society functions is the balance between the rights of an individual to do what they want and the benefit to and protection of society. In the US, we have always tended toward the individual, but public health laws, regulations, rules, and recommendations are based upon the benefit to society. This makes sense because infectious diseases do not limit themselves to only those people who have consciously and willingly made the decision to take the risk of acquiring them. They also affect those who, absent governmental requirements to protect them, are forced to come to work and risk being infected or lose their livelihood, and those who are old or sick but come into contact (even in families) with those who have acquired infection because protecting themselves was just too much trouble.
The logic is flawed; what if laws against killing and stealing were made recommendations to be adopted by those who wished to be cautious? It would not just affect those who made the decision to not adopt them. Sure, we have people killing and stealing and being killed and being robbed despite the laws against it, but those laws protect us far more than a general recommendation that folks not kill or steal would. So too it is with the virus; if you go shopping and few others are wearing a mask despite rules or recommendations that they do, you are at risk. If those rules are repealed and the recommendations rescinded, then more and more people will think they are safe not doing so.
Vaccines are good and protect a lot. They do not by any means eliminate the danger. The changes in recommendations mean the politicians to whom CDC answers will be more popular, and be more likely to get re-elected.
And that more people will die.
