“Mr.
McConnell has always taken pride in protecting his members.” -- NY Times, June 23, 2017
First, let’s start with a reminder about how insurance
works. Money (“premiums”) is collected from everyone, or as many people as
possible, and when the bad thing happens (insurance is almost always about
protecting against bad things, like car accidents, or fires, or death, or
illness), the victims are compensated. If it pays out more than it collects,
then the insurance company goes bankrupt and can no longer pay out. This works
for all types of insurance, whether for-profit (as most is in the US),
not-for-profit (like many health-insurance companies in other countries), or
social insurance where everyone is a client and government is the insurer.
Insurance companies, especially for-profit insurance companies, have to build
in a profit margin as well. In addition, they prefer insure people who are at
low risk of requiring payout, and not to insure or charge higher premiums to
those who are at higher risk (e.g., younger drivers, for car insurance). This
process is known as “underwriting”.
If an insurance company is forced to insure a lot of high-risk
people (as they were under ACA) and can’t charge them really a lot (under ACA they could charge 3 times as much), they
need a lot of low-risk people to pay premiums to be able to fund their probable
payouts; thus the “individual mandate”. For social insurance, such as
government financed health insurance programs (as in many other developed
countries, or Medicare and Federal employee and military programs in the US),
it is actually not necessary that more money come in from premiums than is paid
out, because the government can (if it wishes) subsidize the loss from other
funds. This is, of course, a political decision on how to allocate tax dollars
and how many tax dollars to collect.
 The Senate Republican
leadership has made its position on this completely clear with its recently
unveiled “health care” bill, the “Better Health Care Act” (BHCA). Crafted by
Majority Leader McConnell and a small group of white men from a small group of
places (for example, 2 senators each from Utah, Wyoming, and Texas). It will and
should be called #Trumpcare; while the President didn’t write it, he has
endorsed it and will sign it if it passes the Senate and the House
reconciliation. It is clearly a tax-cut-for-the-wealthy bill that derives
funding from the reduction (and sometimes elimination) of health care coverage
for a very large percent of Americans; this is detailed by the NY Times’ Margot Sanger-Katz in “Shifting
Dollars From Poor to Rich Is a Key Part of the Senate Health Bill”, June
22, 2017. The Times also has a piece
by Sanger-Katz and Haeyoun Park that contains a clear listing of what will be
cut from the ACA in order to fund these tax cuts, “How
Senate Republicans plan to dismantle Obamacare”, summarized in the graphic.
However, the details are important; even the parts of the ACA that the BHCA “keeps”
are largely undercut by other parts of the bill. For example, it keeps the
requirement that insurers must issue policies to people with pre-existing conditions (which can range from heart
disease and cancer to endometriosis and broken bones and everything else),
which is good. But it raises the amount that insurers can charge these people
from 3 times as much under ACA to 5 times as much. This is a big deal, and a
bad deal, for people with disabilities and for older people who are, (surprise!),
much more likely to have pre-existing conditions.
The Senate Republican
leadership has made its position on this completely clear with its recently
unveiled “health care” bill, the “Better Health Care Act” (BHCA). Crafted by
Majority Leader McConnell and a small group of white men from a small group of
places (for example, 2 senators each from Utah, Wyoming, and Texas). It will and
should be called #Trumpcare; while the President didn’t write it, he has
endorsed it and will sign it if it passes the Senate and the House
reconciliation. It is clearly a tax-cut-for-the-wealthy bill that derives
funding from the reduction (and sometimes elimination) of health care coverage
for a very large percent of Americans; this is detailed by the NY Times’ Margot Sanger-Katz in “Shifting
Dollars From Poor to Rich Is a Key Part of the Senate Health Bill”, June
22, 2017. The Times also has a piece
by Sanger-Katz and Haeyoun Park that contains a clear listing of what will be
cut from the ACA in order to fund these tax cuts, “How
Senate Republicans plan to dismantle Obamacare”, summarized in the graphic.
However, the details are important; even the parts of the ACA that the BHCA “keeps”
are largely undercut by other parts of the bill. For example, it keeps the
requirement that insurers must issue policies to people with pre-existing conditions (which can range from heart
disease and cancer to endometriosis and broken bones and everything else),
which is good. But it raises the amount that insurers can charge these people
from 3 times as much under ACA to 5 times as much. This is a big deal, and a
bad deal, for people with disabilities and for older people who are, (surprise!),
much more likely to have pre-existing conditions.
While BHCA (Trumpcare) repeals the individual mandate, which
will make some people happy (until they get sick) and the employer mandate
(which will make employers happy), it also repeals the subsidies for
out-of-pocket costs and decreases funding for subsidies to make policies on the
exchanges affordable. The new bill would make either premiums or deductibles
(or both) unaffordable for many Americans. It limits and sometimes eliminates
the requirement that insurers provide “essential health benefits”, like
preventive care and contraception, allows insurers to set annual and lifetime
limits on how much they have to pay, and makes major negative changes to
Medicaid. Medicaid is currently largely paid for by the federal government,
50%-80+% depending on the average state income, and 90-100% for people covered
by Medicaid expansion. The “changes” include (gradually, so the impact won’t be
seen for the 2018 election) cutting and capping the amount the federal
government pays, shifting costs to the states, which often will not be able (or
willing) to cover them.
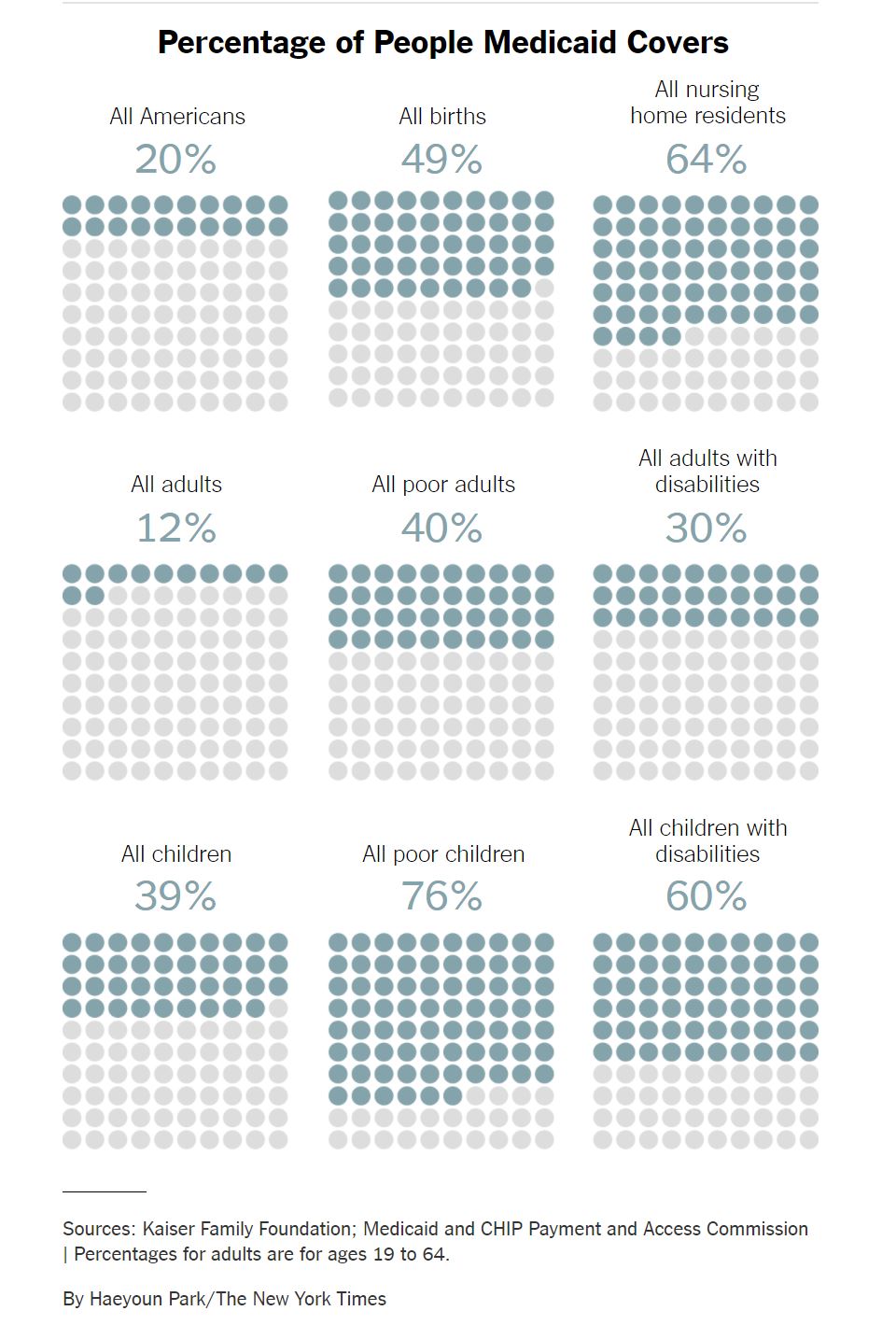
This will affect a lot of people. Medicaid is now the
largest insurer in the US, covering 69 million Americans, even though many
states did not expand it under the ACA to cover poor adults. What it does is
summarized in “How
Medicaid works and who it covers” by Abby Goodnough and Kate Zernike. It
covers, as seen in the accompanying chart, 79% of poor children (and more than a
third of ALL children), 64% of nursing home patients (many of whom were middle
class before the NH wiped out their savings!), 60% of children with disabilities,
49% of births, 30% of adults with disabilities. The people who will suffer from Medicaid cuts are old people in nursing
homes, children, and disabled people (many of whom are able to stay in the community
and even keep jobs rather than being in nursing homes because of this support). With
the caps on lifetime benefits, it means, as
Dr. Eve Shapiro points out in an Op-Ed in the Arizona Daily Star, “that a premature baby on private insurance
could exceed her lifetime limit on coverage before she even leaves the hospital”!
And, with the right convergence of decisions by the state, the same could happen
to an infant with Medicaid.
This is a big deal. Ideologues and pundits and politicians like
to debate theoretical issue to see who scores the most points. They want to be
the “most conservative”, the most “anti-abortion”, the most “pro-industry”, the
most “anti-tax”. If they are articulate they may think that making their smarmy
points makes them win. And I guess it does. Except the losers are not those on
the other side of a debate podium, they are the majority of the American
people, the politicians’ constituents, who don’t get treatments, don’t get
diagnosed, do get sick and die. Lives, not ideologies, are at stake.
Except, of course, it is about ideology. This is made clear
in “A
debate that shows what each party cares about” by Neil Irwin the Times. No one, certainly not a senator
who has to run for re-election, wants to say that they are about making it
harder or impossible for many (often the majority) of their constituents to be
able to access health care, or to pay for it, or to get the treatments and
therapies they need. But make no mistake: every senator who votes for this bill
is saying exactly that, that they value tax cuts for the most privileged above
basic health care for the rest of us. “This plan will improve the affordability
of health insurance,” lied Sen. McConnell in a recent
opinion piece in the Cincinnati paper.
Yes, “Mr. McConnell
has always taken pride in protecting his members.” And his donors. It is
too bad that he has no interest in protecting the rest of us.



